

I Published the Brainstem Hypothesis of Long Covid in 2021. New Studies Now Validate It
An idea once overlooked is now gaining recognition in Long Covid research.

In 2021, I published an academic paper on an idea that sounded almost too strange to take seriously: Long Covid might be mainly a brainstem problem. At the time, it was just a hypothesis based on patterns I noticed in autopsy studies on the distribution of SARS-CoV-2 in the brain, as well as the overlapping functions of the brainstem with symptoms of Long Covid.
In the past year, however, several high-quality studies have been pointing in the same direction. If the brainstem really is at the heart of Long Covid, it could explain why the illness is so bewildering, why its symptoms are so wide-ranging, and why doctors have struggled to pin it down.
Looking Back Five Years
We all remember it: the World Health Organization’s alarm that declared Covid-19 as a pandemic in March 2020. The world’s attention shifted almost overnight. Research priorities flipped, news cycles were consumed, and soon another phrase began circulating — Long Covid.
I was no different. At that time, I was an amateur neuroscientist and blogger, locked out of university labs like everyone else. With the extra time I had, I started researching and writing about Covid-19, trying to make sense of the unfolding crisis and sea of information (and misinformation).
Because I was immersed early, I noticed the growing Long Covid problem in the real world before many in academia did. I blogged about it, then turned those insights into some of the first peer-reviewed papers on the subject, including the brainstem hypothesis of Long Covid.
These early papers are still widely cited to this day, even earning me a spot in Stanford’s list of top 1% most-cited scientists from 2022 to 2024 and a current ranking of #31 in Long Covid research in Google Scholar.
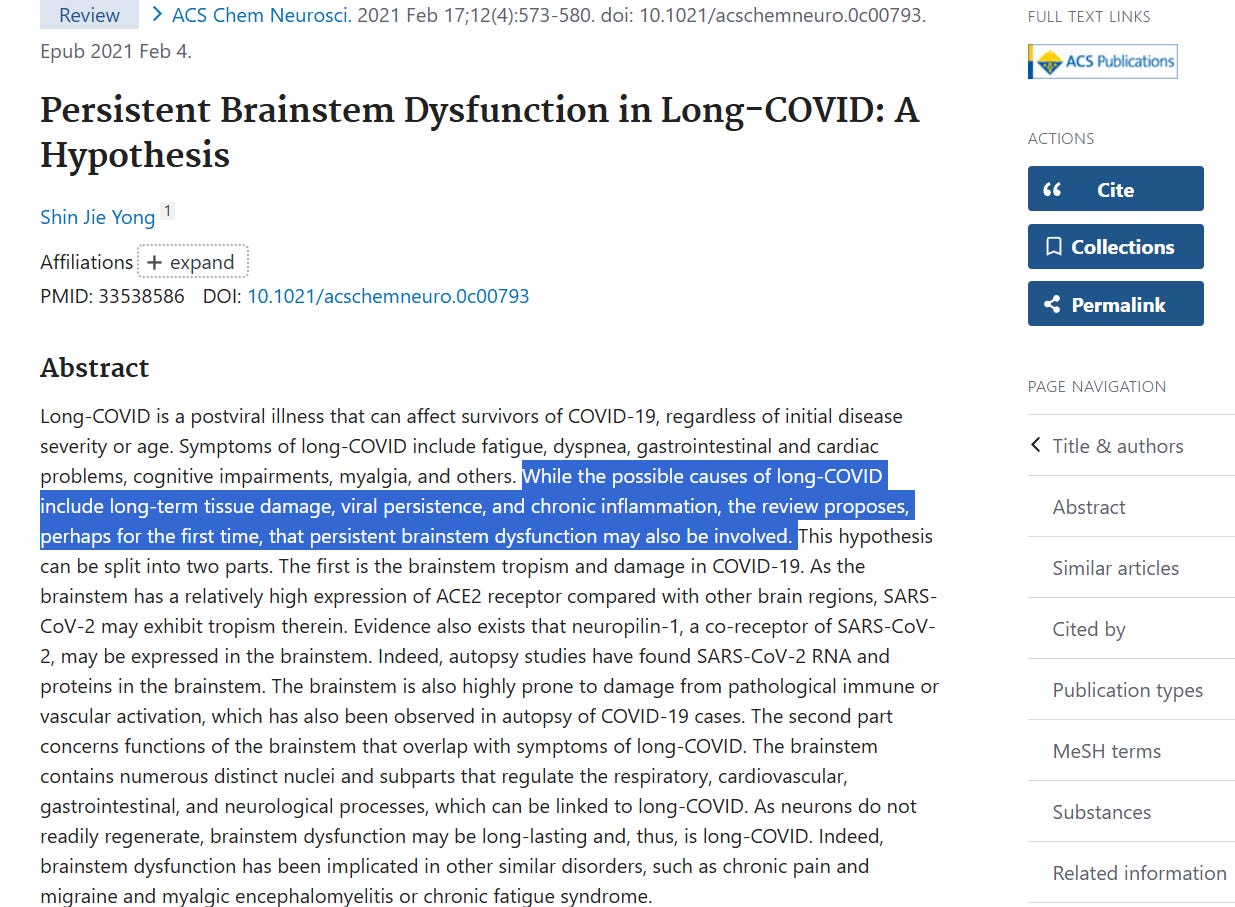
Now, let me tell you about the brainstem hypothesis of Long Covid that fascinated me in late 2020, which I drafted and published in ACS Chemical Neuroscience in February 2021. If I’m not mistaken, this was the first paper to formally propose the brainstem hypothesis of Long Covid (Figure 1).
The Brainstem Hypothesis of Long Covid
The myriad symptoms of Long Covid—fatigue, brain fog, breathlessness, racing heart, dizziness, gut upset, and unrefreshing sleep, among others—look chaotic until you ask two simple questions:
Where does SARS-CoV-2 travel in the brain, and which regions does it tend to affect?
What single control hub could produce such a wide and overlapping range of symptoms if disrupted?
In my 2021 paper, I argued that both questions point to the brainstem. Even subtle or lingering dysfunction in this brain region—triggered by viral infection or inflammatory injury—could plausibly induce the diverse and persistent symptom set of Long Covid.
Let me walk you through the evidence in two parts.
I. SARS-CoV-2 Distribution in the Brain
SARS-CoV-2 gains entry into human cells through the ACE2 receptor. So, any cell displaying ACE2 on its surface is a potential target.
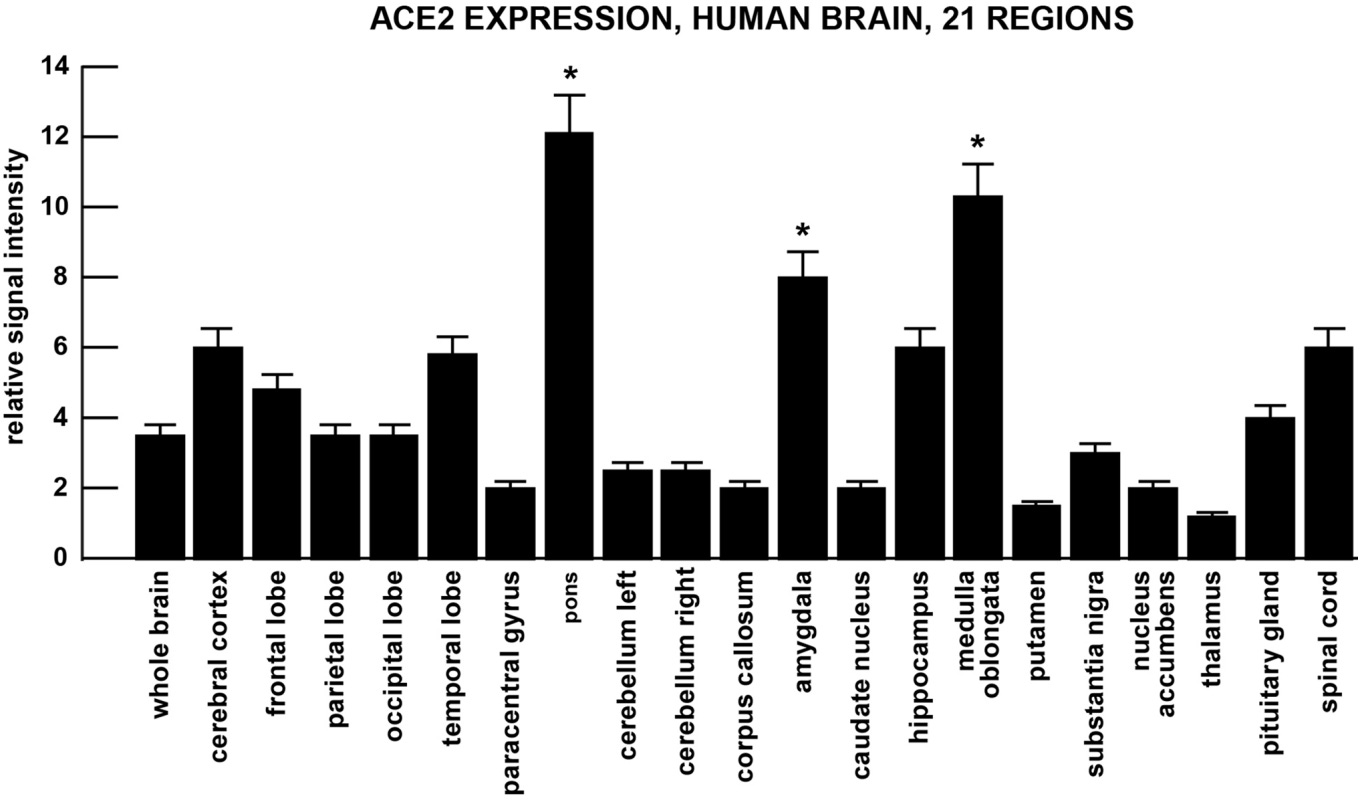
To better understand the spectrum of cells that SARS-CoV-2 can infect, Lukiw et al. at Louisiana State University Health Sciences Center, New Orleans, systematically measured ACE2 expression across 85 different human tissues, including 21 brain regions.
As expected, ACE2 was abundant in the lungs, gut, kidneys, and heart. But the surprise was the brain. The highest levels appeared in the brainstem, specifically the pons and medulla oblongata, which serve as the control centers for breathing and heart function (Figure 2). This receptor map provides a molecular rationale for why some Covid-19 patients develop respiratory failure that can’t be explained by lung damage alone. The virus might have attacked the brain circuits that regulate breathing.
That said, is there evidence of SARS-CoV-2 infection in the human brain, particularly the brainstem? The only way to answer that question is through autopsies. As we can’t just cut open a living human brain to find traces of the virus, autopsy examinations of brain tissue from patients who died with Covid-19 are our best source of direct evidence.
One of the earliest autopsy studies on the brains of people who died with Covid-19 came from the University Medical Center Hamburg-Eppendorf, Germany. Published in Lancet Neurology in late 2020, Matschke et al. examined multiple brain regions for the presence of neuroinflammation and SARS-CoV-2 genetic or protein fragments.
While signs of immune activation were seen across the brain, the brainstem and cerebellum showed the strongest signs of neuroinflammation. Microglia (the brain’s immune cells) were activated, and inflammatory T-cells had infiltrated these brain regions. In 53% of cases, SARS-CoV-2 protein fragments were also detected, often in the brainstem or the cranial nerves of the lower brainstem. The overall brain damage was mild, but the brainstem stood out as a hotspot for neuroinflammation and viral presence.
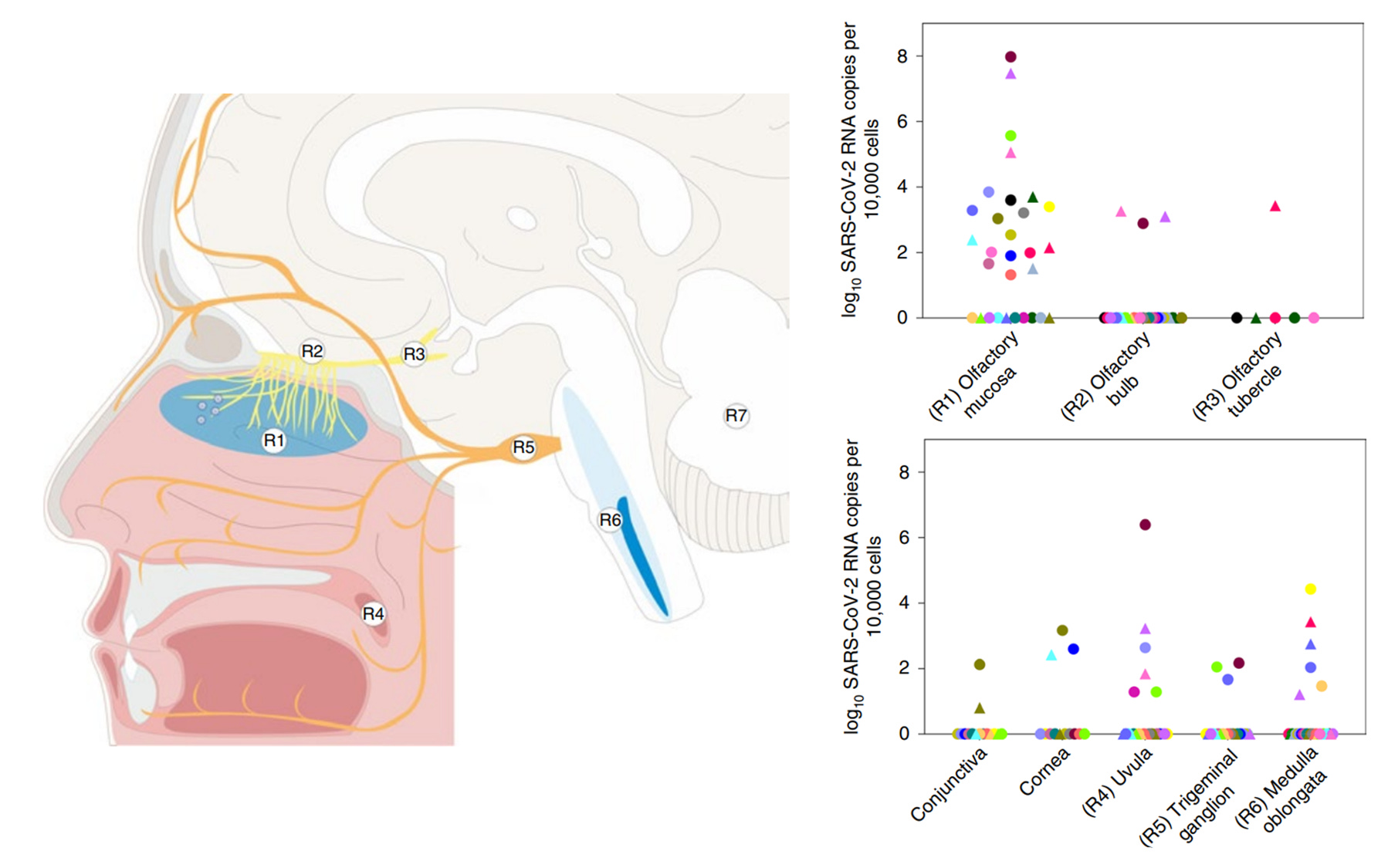
Another German study provided compelling evidence for the infection trajectory pathway of SARS-CoV-2 in the brain. Published in Nature Neuroscience in 2021, Meinhardt et al. from Humboldt University of Berlin and the Berlin Institute of Health, mapped the presence of SARS-CoV-2 genes and proteins across the nasal passages, cranial nerves, and multiple brain regions in an autopsy of 33 patients who died with Covid-19.
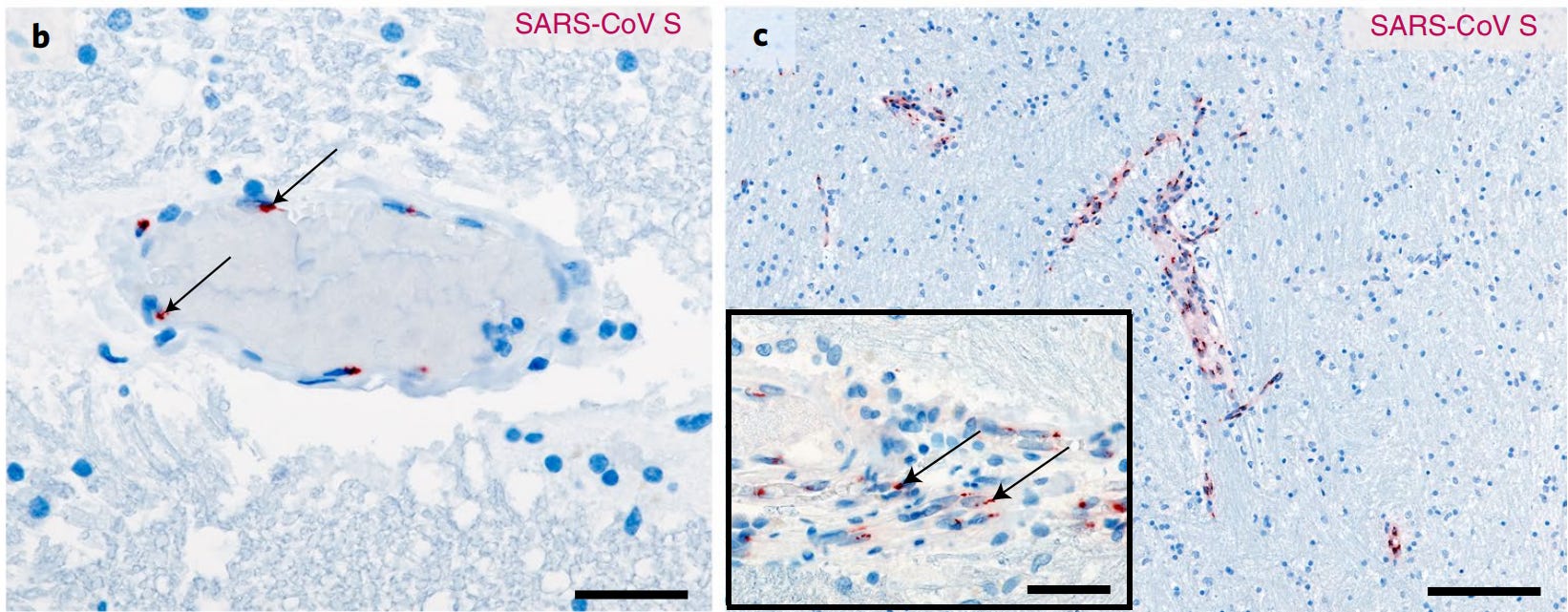
The highest viral loads were found in the smell-sensing olfactory mucosa. From there, the virus followed an anatomical pathway inward, being found in the olfactory bulb, trigeminal ganglion, and medulla oblongata of the brainstem (Figure 3). Signs of neuroinflammation were also observed, with activated microglia clustering in brainstem regions.
What made the study compelling was the use of multiple methods to detect the genes (in situ hybridization), proteins (immunohistochemistry), and even virion particles (electron microscopy) of SARS-CoV-2 (Figure 4). While these methods did not always align perfectly, and not every patient sample was positive for SARS-CoV-2, they converged on a consistent pattern: the nose was the entry site, and the brainstem was the target.
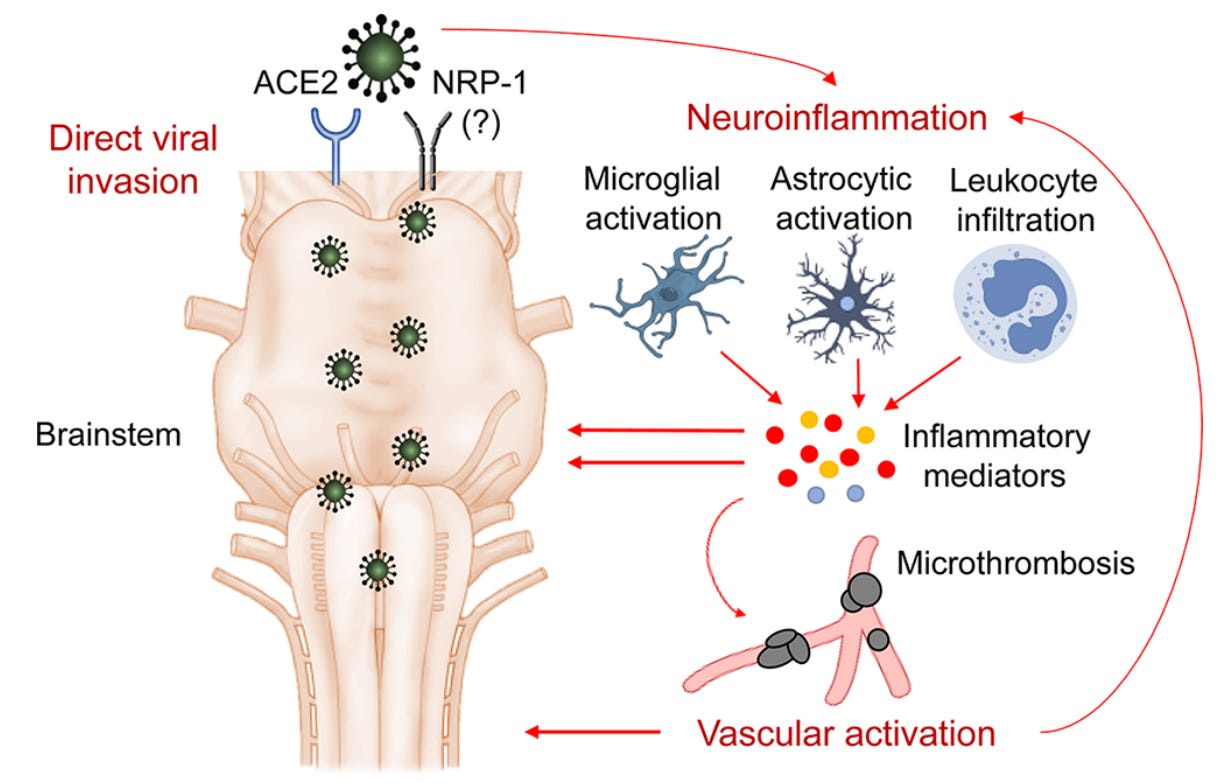
In my 2021 paper, I also highlighted other autopsy studies finding brainstem abnormalities despite the absence of SARS-CoV-2 fragments. The abnormalities include immune cell infiltration, microglia activation, and even tiny blood clots (microthrombi) in the brainstem. These studies suggest that, in addition to direct viral invasion, Covid-19 can damage the brainstem indirectly via immune and vascular routes (Figure 5).
II. Brainstem as the Body’s Control Hub
By now, you might be wondering: What exactly is the brainstem, and why does it matter so much for Long Covid?
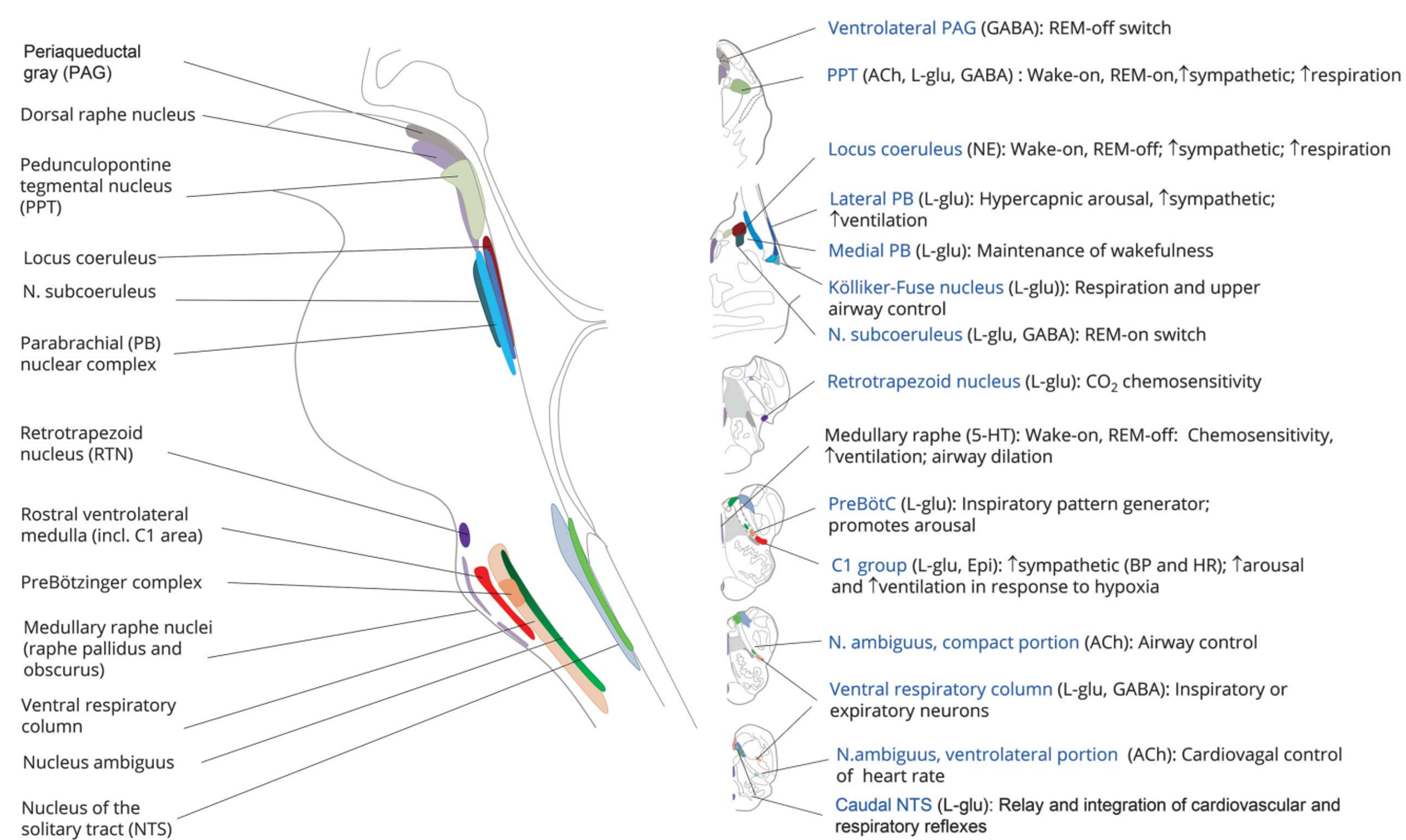
The brainstem—made up of the midbrain, pons, and medulla oblongata—is sometimes called the body’s autopilot. It’s a compact structure, but it quietly oversees many of the functions that keep us alive without conscious effort: breathing, heart rate, blood pressure, sleep-wake cycles, gut motility, swallowing, and even pain and mood regulation (Figure 6).
Here are the specifics:
Breathing control: Neurons in the medulla oblongata (specifically the Bötzinger and pre-Bötzinger complexes) generate the rhythm of every breath, while circuits in the pons (pontine respiratory group) smooth the transition between inhaling and exhaling.
Heart control: The caudal ventrolateral medulla (CVLM) regulates heart rhythm and blood pressure, keeping the cardiovascular system in sync.
Gut regulation: The nucleus tractus solitarius (NTS) and dorsal motor nucleus of the vagus (DMV) connect the brainstem to the gastrointestinal tract via the vagus nerve, which regulates gut motility, secretion, and reflexes, such as nausea and vomiting.
Taste (and smell) alterations: Gustatory neurons in the NTS carry taste signals to the brain’s higher centers. Damage to the olfactory-brainstem pathway may explain the concomitant loss of smell.
Sleep and alertness: The reticular activating system (RAS) in the pons governs sleep–wake cycles and attention, disturbances of which contribute to insomnia, fatigue, and brain fog.
Neurotransmitter supply: The brainstem is the source of many neurotransmitters: serotonin (produced in the raphe nuclei), noradrenaline (locus coeruleus), and dopamine (ventral tegmental area and substantia nigra). Disruption here can ripple outward, affecting mood, anxiety, cognition, pain, and energy.
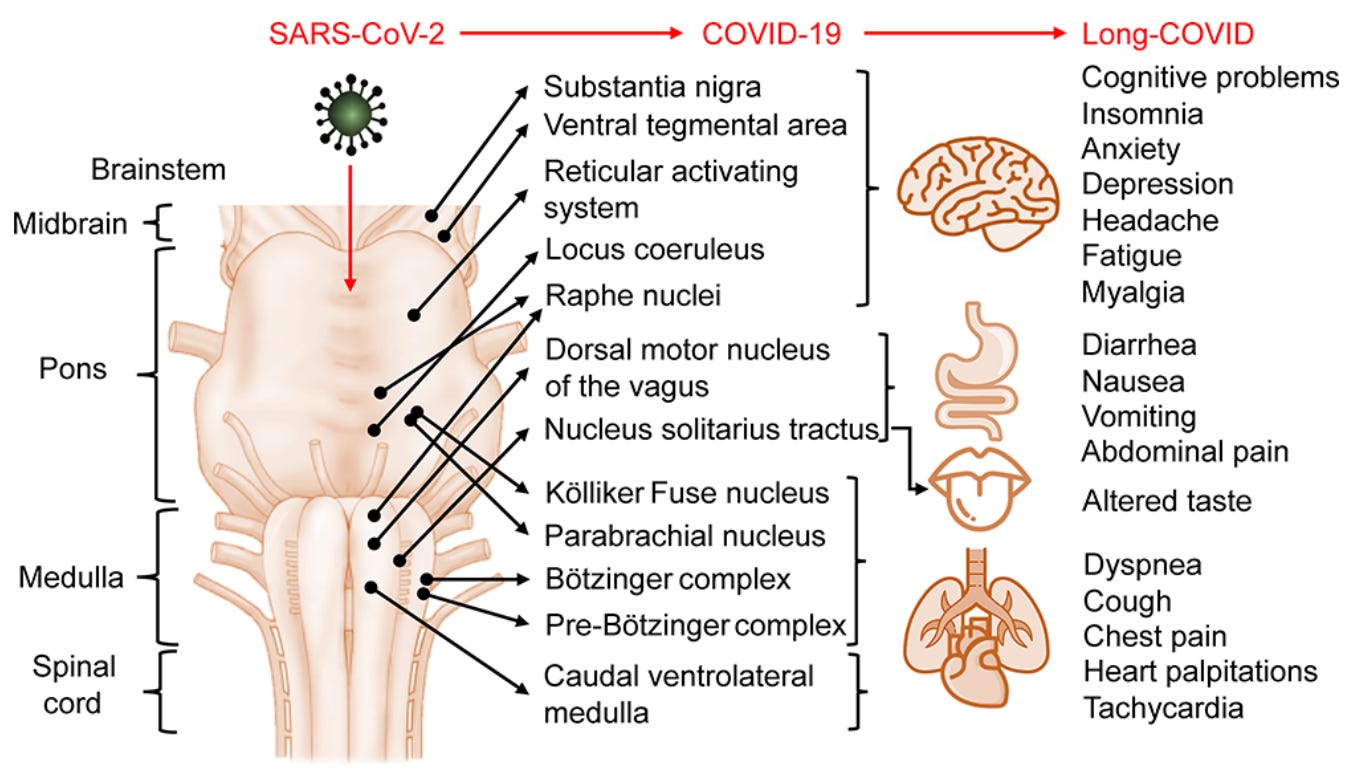
Because the brainstem is such a densely packed control center, even subtle dysfunction can have far-reaching effects. Disturb its circuits, and you don’t just get one symptom but many at once: shortness of breath, heart palpitations, dizziness, gut upset, insomnia, fatigue, and brain fog.
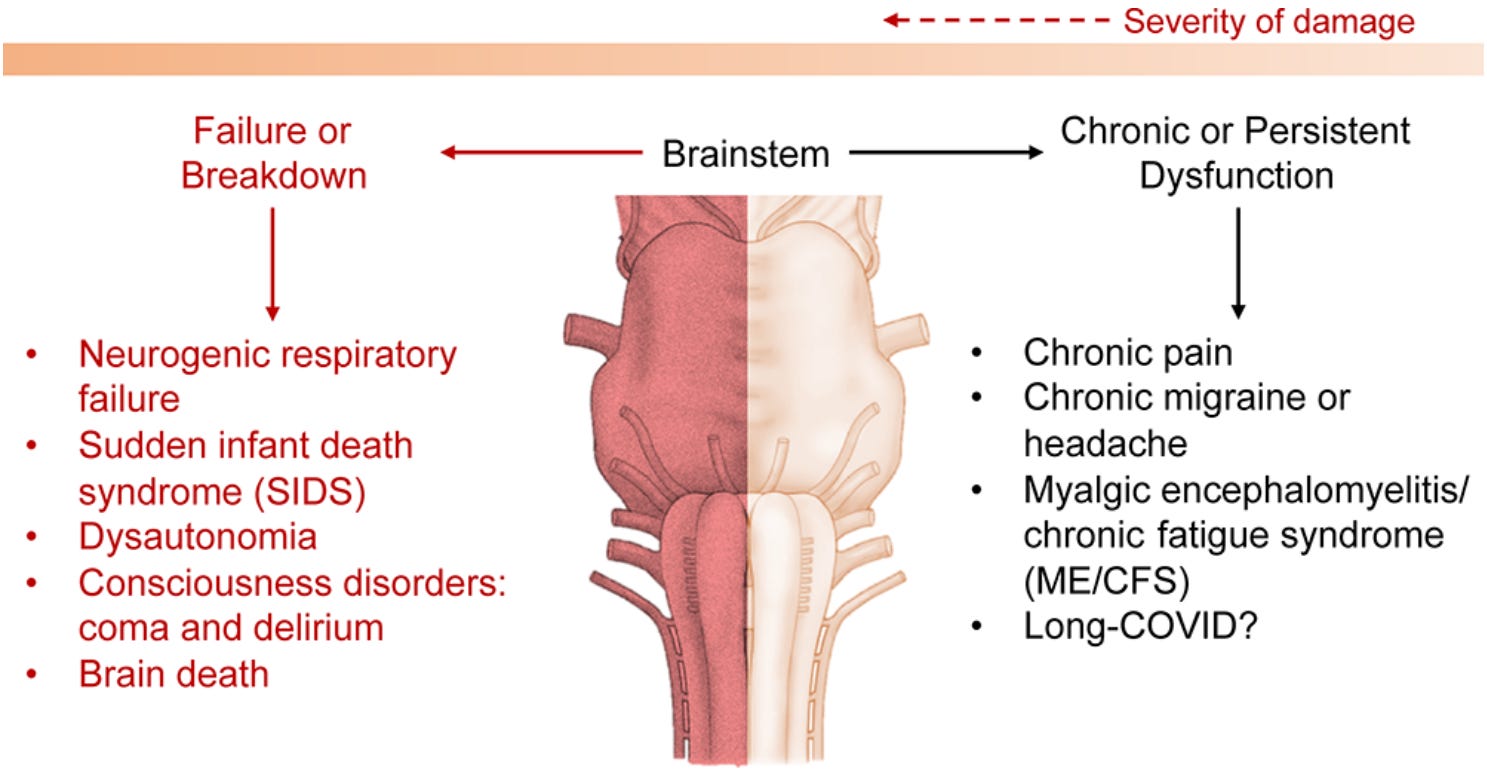
In other words, the very same tangle of symptoms of Long Covid can, in theory, be generated by low-grade brainstem dysfunction (Figure 7).
I mentioned low-grade dysfunction because severe brainstem damage is deadly. Disruption to the brainstem’s pre-Bötzinger complex, the respiratory pacemaker, can lead to neurogenic failure and death. Traumatic impact or physical injury to the brainstem also carries a high mortality rate. And conditions like sudden infant death syndrome are thought to stem from failure of the brainstem serotonin circuits.
In other words, if Long Covid were caused by major brainstem damage, most patients would not survive.
But evidence from other similar chronic disorders shows that the brainstem can also malfunction in subtle, non-lethal ways.
Brain imaging studies have found altered connectivity in the brainstem of people with chronic pain and migraine. Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), a condition that highly overlaps with Long Covid, has also been linked to brainstem dysfunction.
A 2020 systematic review of 63 brain imaging studies in ME/CFS patients found that the brainstem often emerged as abnormal, with studies reporting structural changes, altered blood flow, impaired functional responses, and even signs of neuroinflammation in the brainstem.
These precedents suggest that even low-grade disruption of brainstem circuits could explain the persistent, multisystem symptoms of Long Covid. In this manner, Long Covid may not be a completely new mystery, but rather part of a continuum of brainstem disorders (Figure 8).
Emerging Clinical and Biological Evidence
This is where things get more interesting and definitive. Since February 2021, when I published the brainstem hypothesis of Long Covid paper, several studies have supported this hypothesis. I’ll describe the emerging evidence in, again, two parts: clinical and biological.
I. Clinical Evidence from Human Brain Scans
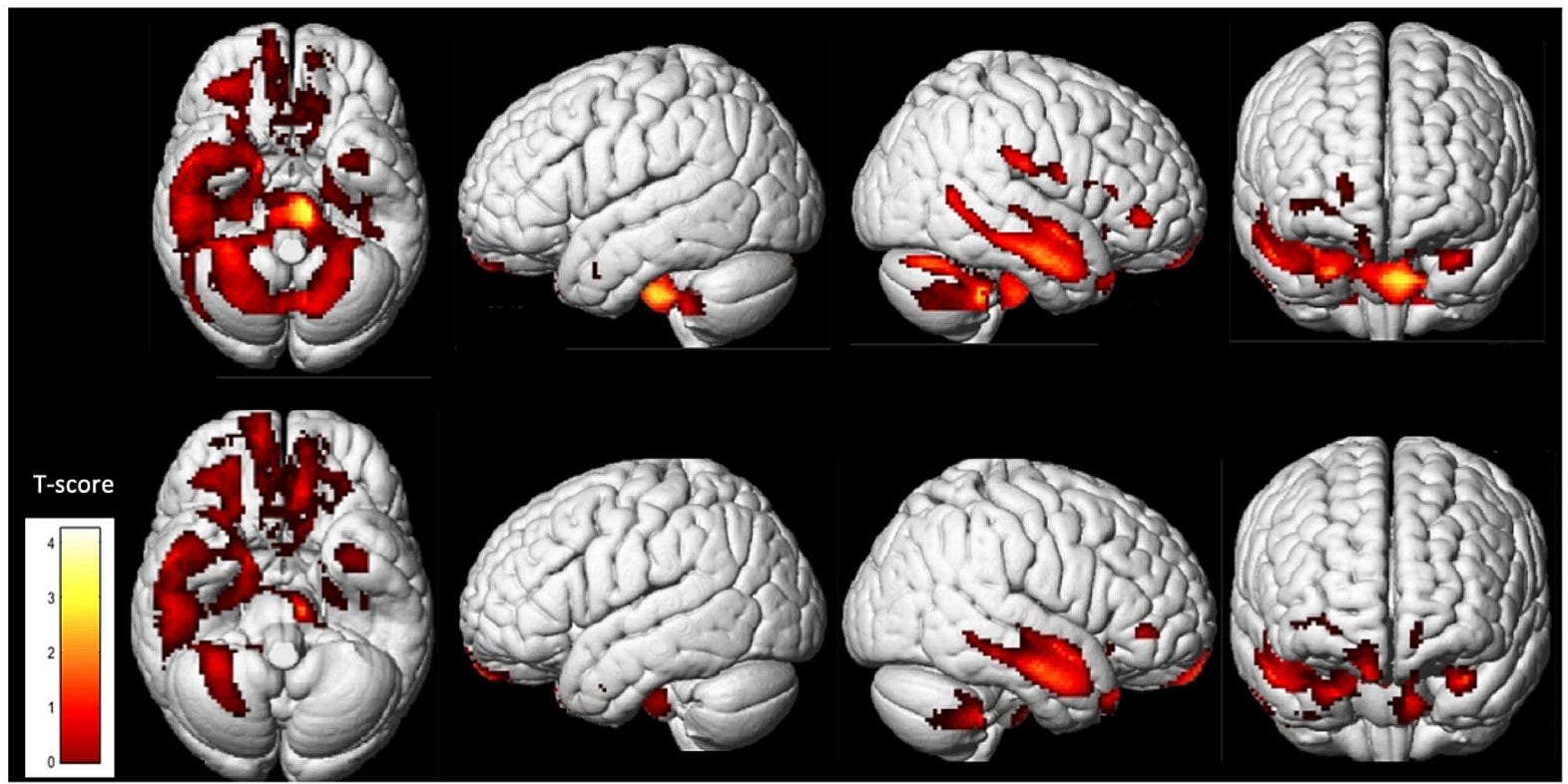
Not long after I published my 2021 paper, Guedj et al. at Aix-Marseille University, France, reported that brain imaging of Long Covid patients showed hypometabolism (reduced energy use) in parts of the brainstem (pons and medulla), as well as the limbic, cerebellar, and olfactory regions. Importantly, the degree of brainstem and cerebellar hypometabolism correlated with the severity of patients’ symptoms.
Since then, at least three other studies have replicated this pattern in both adults and children with Long Covid. One of them, a 2024 longitudinal study from the same French research group, scanned patients’ brains twice, nearly a year apart. As expected, persistent hypometabolism was observed in the brainstem’s pons and cerebellum, with little to no signs of recovery (Figure 9). These studies thus reinforce that impaired energy use in the brainstem and cerebellum is a hallmark of Long Covid.
Building on this, Rua et al. (2024) from the University of Cambridge and University of Oxford applied quantitative susceptibility mapping (QSM), an MRI method that detects subtle tissue changes, such as inflammatory injury and iron deposition. And they reported abnormalities in the brainstem areas (medulla and pons) among Covid-19 survivors who were scanned 6–7 months after hospitalization. These abnormalities were linked to more severe Covid-19 and poorer recovery thereafter.
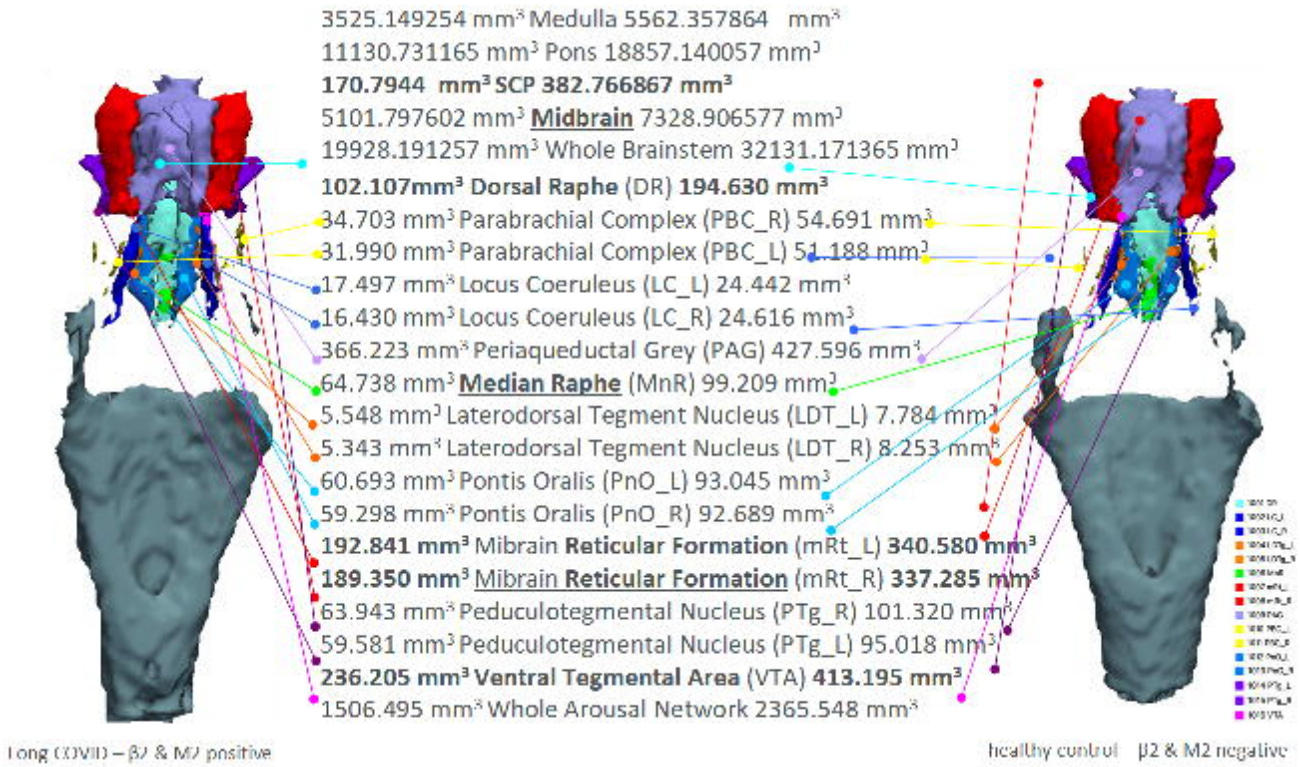
Most recently, Christof et al. (2025), an international team from Poland, Germany, South Africa, and the U.K., pushed the field forward by showing that the brainstem is not only metabolically impaired but also structurally altered in Long Covid. They used advanced MRI morphometry, a brain scan technique that enables precise volume and shape measurements, in a group of 44 Long Covid patients and 14 healthy controls. And they first released their paper as a preprint (not yet formally published).
First, they found significant volume loss in the medulla and pons areas of the brainstem — the same regions identified as metabolically underactive (hypometabolic) in prior brain imaging studies. There was also volume loss in the dorsal raphe and midbrain reticular formation, which are brainstem regions that regulate pain and the sleep-wake cycle (Figure 10).
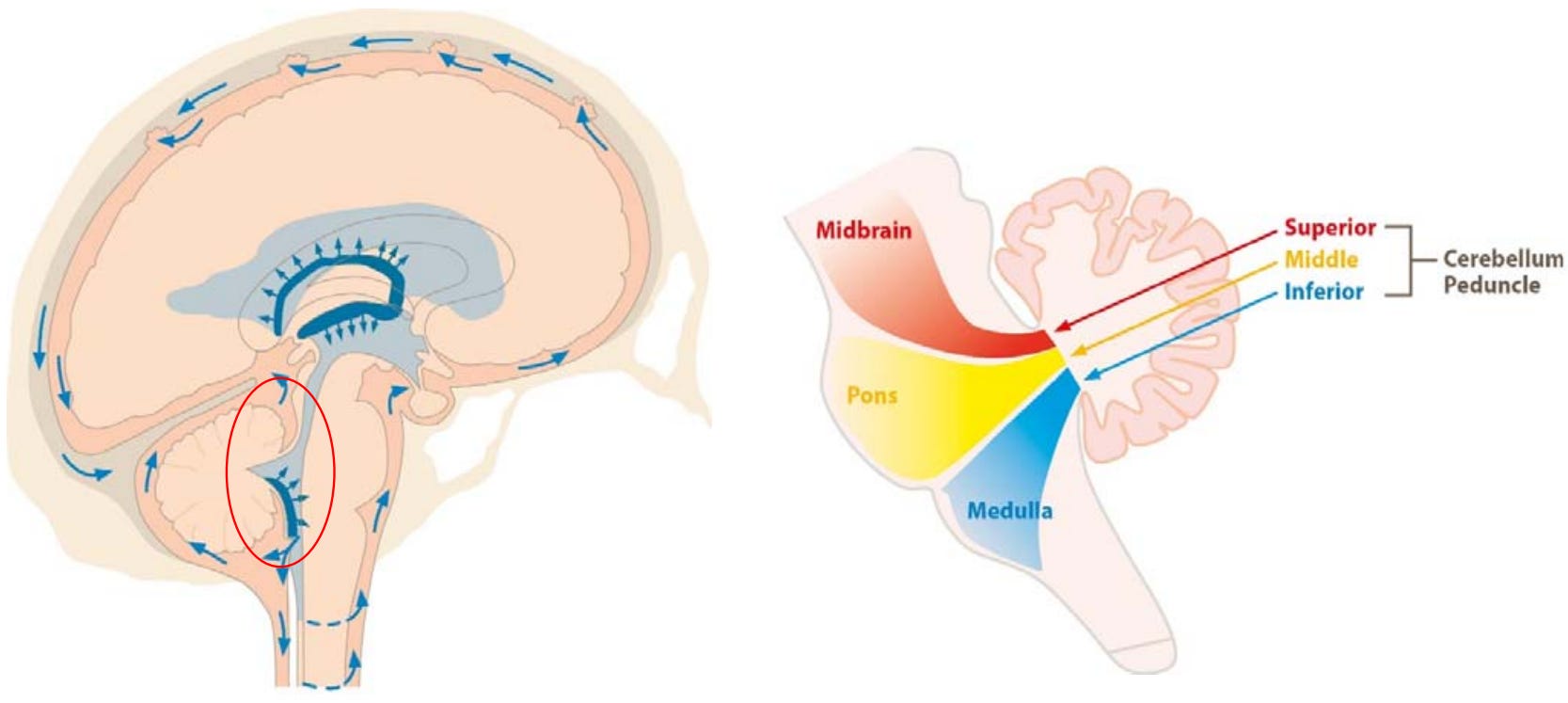
What’s more interesting is that Christof et al. detected subtle deformations in a crucial area connecting the brainstem to the cerebellum: the cerebellar peduncle of the fourth ventricle (Figure 11). Volume reductions were noted in the superior cerebellar peduncle, as well as compromised white matter integrity in the middle cerebellar peduncle (Figure 10).
In practical terms, this suggests that Long Covid disrupts not just the brainstem itself but also its communication highways with the cerebellum, undermining the circuits that coordinate movement, posture, and autonomic control. Christof et al. called this the “Broken Bridge Syndrome.”
More importantly, the degree of this broken bridge correlated with key symptom clusters of Long Covid, including motor deficits, sensory dysfunction, and autonomic dysregulation (where the autonomic nervous system — which regulates involuntary organ functions such as breathing, heart rate, blood pressure, and digestion — is impaired).
(II) Biological Evidence from Animal Models
While human brain scans point to brainstem abnormalities in Long Covid, animal models allow us to investigate what’s actually happening at the biomolecular level.
In a new study published in Nature Communications, Coleon et al. from the Pasteur Institute in France developed a golden hamster model of Long Covid and provided some of the strongest biological evidence yet that the brainstem is directly involved.
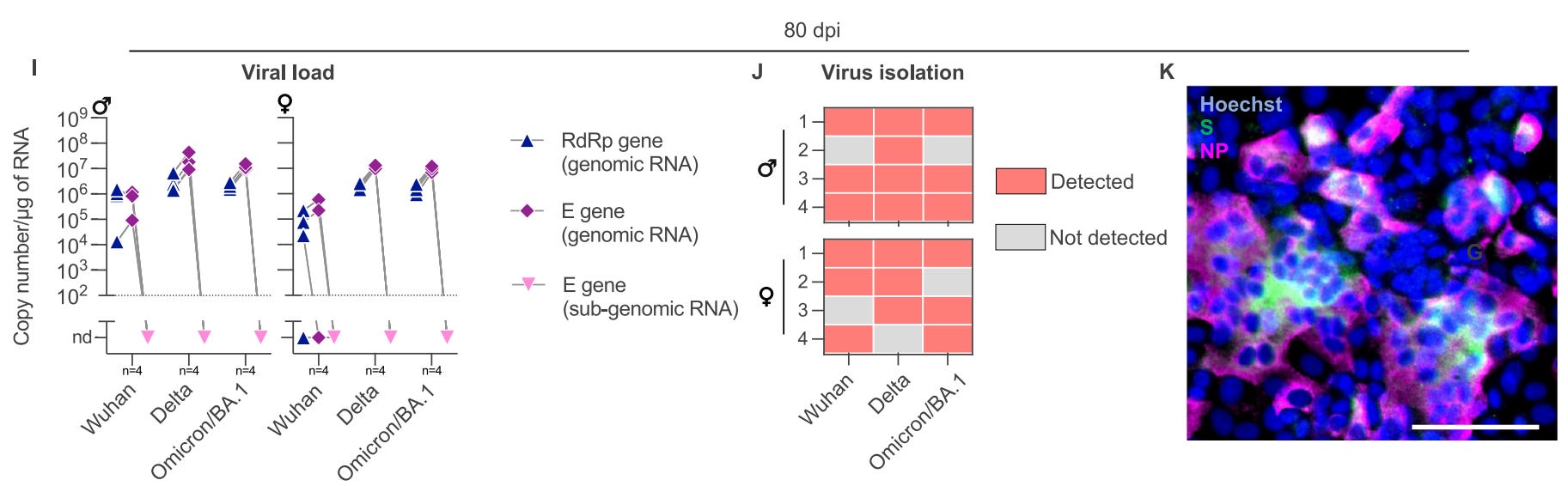
They found that SARS-CoV-2 infected the hamster brainstem within hours of nasal infection and persisted there for at least 80 days, the equivalent of several years in human time. More convincingly, Coleon et al. successfully isolated infectious virus particles from the brainstem months after the initial illness, indicating that the brainstem can act as a long-term viral reservoir (Figure 12). Other brain regions showed inconsistent or no traces of SARS-CoV-2 genetic material. So, the brainstem is the only site where both viral fragments and infectious virus persisted.
As the authors wrote, “Surprisingly, we report the unprecedented isolation of infectious viral particles from the brainstem of hamsters with long COVID 80 days after infection, regardless of sex and SARS-CoV-2 variant.”
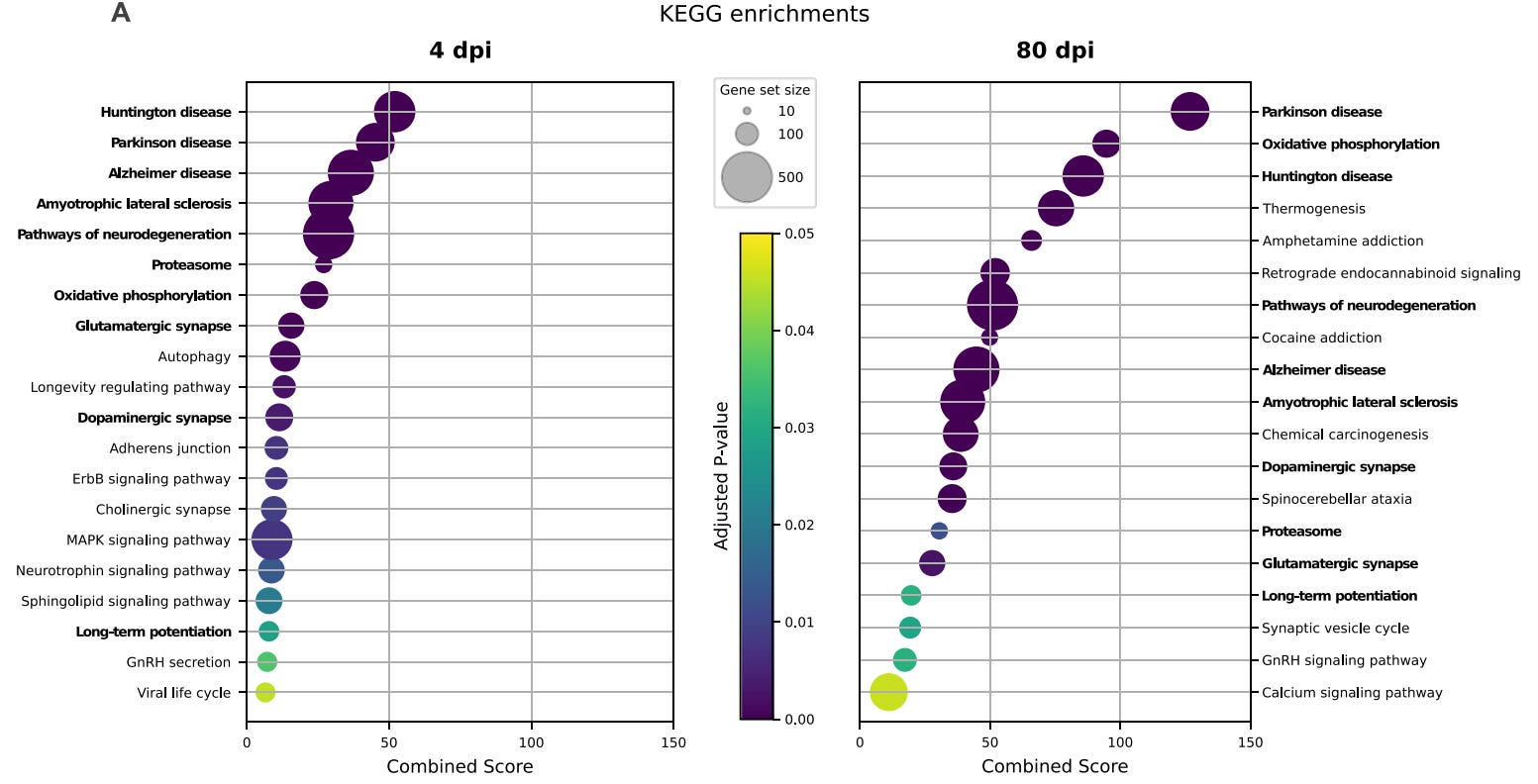
At the molecular level, the brainstem of infected hamsters exhibited a neurodegenerative-like signature. Genes involved in energy production, protein quality control, and synaptic signaling were disrupted in ways similar to those observed in common neurodegenerative diseases, such as Parkinson’s and Alzheimer’s diseases (Figure 13). The brainstem’s neurotransmitter systems were also disrupted, particularly the dopamine and glutamate circuits (essential for movement, motivation, and cognition), as well as the serotonin and acetylcholine circuits to some extent.
Importantly, the hamsters also developed behavioral changes that resemble Long Covid in humans: depression, memory impairment, and late-onset anxiety. Taken together, this work demonstrates that lingering brainstem dysfunction is not just a hypothetical idea, but a biologically plausible mechanism for the persistent symptoms of Long Covid.
Where Do We Go From Here?
The brainstem hypothesis does not claim that every Long Covid case is a brainstem problem, especially since Long Covid itself encompasses a variety of conditions, such as myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), postural orthostatic tachycardia syndrome (POTS), and post-ICU syndrome, each with distinct pathophysiology.
Instead, it proposes that the brainstem is a vulnerable control hub where direct viral, inflammatory, or vascular damage can converge to produce the multi-system symptom web in some cases of Long Covid.
If brainstem dysfunction drives Long Covid for some people, then the next logical question is: can we actually restore its function?
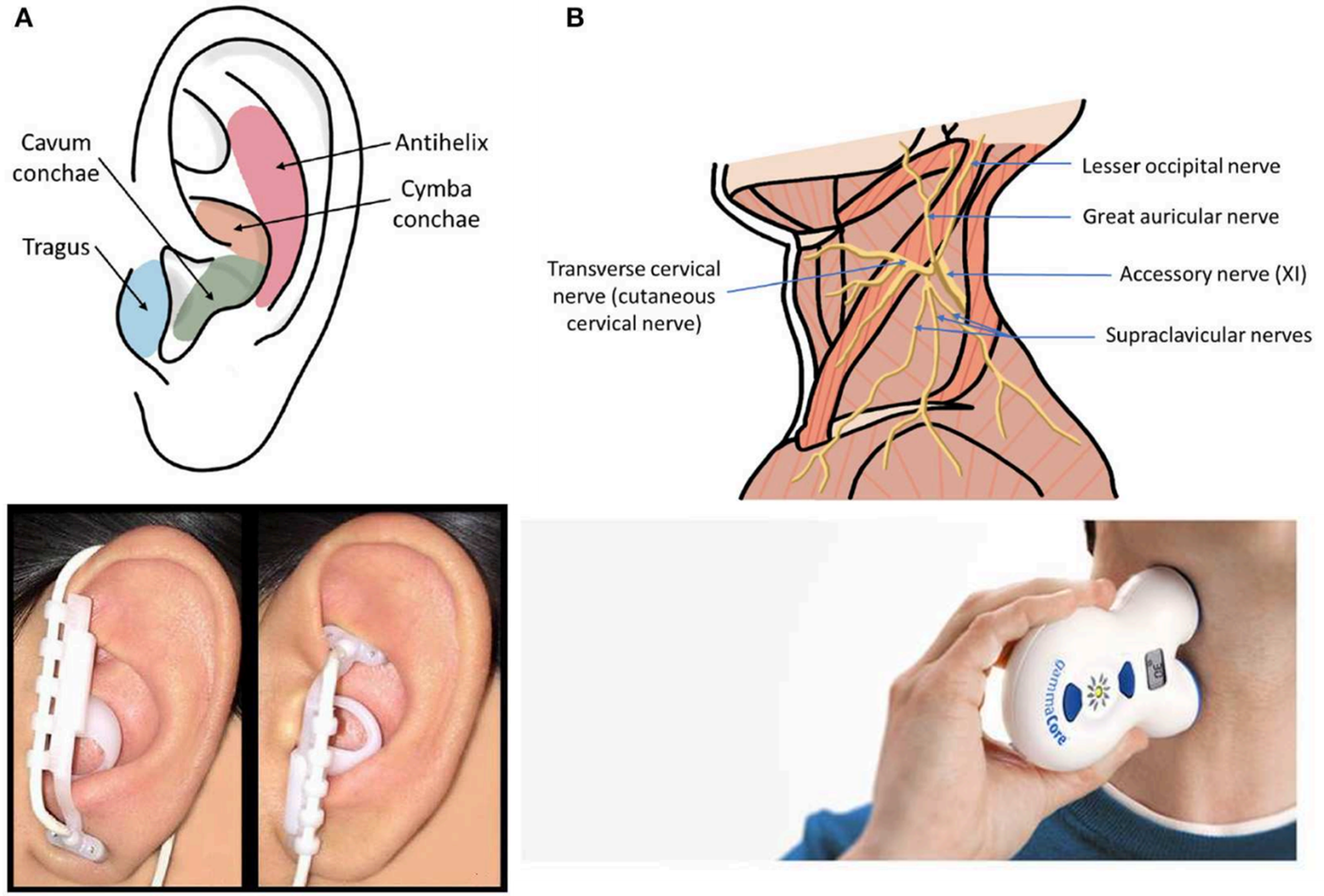
It’s a challenging question because we know little about how to treat brain dysfunction, especially when it involves the brainstem. But it may be possible. The most promising approach for this purpose is a low-risk, non-invasive transcutaneous vagus nerve stimulation (tVNS). The vagus nerve directly connects to brainstem hubs that regulate breathing, heart rhythm, and autonomic balance. By sending electrical pulses through a small device applied to the ear or neck, researchers can “nudge” these brainstem circuits back toward normal function (Figure 14).
A pilot clinical study in Long Covid patients has already reported improvements in symptoms with tVNS, and larger clinical trials are now underway to test this more rigorously.
Even so, it is unclear what tVNS actually does at the neural level. The vagus is a mixed nerve, with 80% of its fibers carrying sensory signals from the body to the brain and the rest sending commands back to organs. When stimulated, the first relay is usually the nucleus tractus solitarius (NTS) in the medulla, which then projects to other brainstem hubs. But since 20% of the vagus nerve connects to other organ systems, including the heart, lungs, and gut, tVNS may also indirectly reshape their functions.
In the end, even if we have pinpointed brainstem dysfunction as one probable driver of Long Covid, we still know very little about how to treat or rehabilitate the brainstem itself. Yet science is always progressing. Five years ago, the brainstem hypothesis of Long Covid I proposed was just a conjecture, without the clinical scans and biological evidence we now have. Five years from now, we may look back and see today’s uncertainties as the first steps toward real answers—and perhaps, real treatments.
If you've made it this far, thank you for reading! Most of my Substack articles are paywalled, so if you found this valuable, consider subscribing for just $2.90/month (annual plan). Your support allows me to dedicate more time to researching and writing about lesser-known but important topics like this.
Update: I’ve written a follow-up on the use of vagus nerve stimulation for Long Covid here: Vagus Nerve Stimulation for Long Covid: Does It Work?